
It is perhaps unsurprising that we would find ourselves in a bit of the doldrums over the last few weeks.
It’s pretty normal in the world of expat psychology, where at some point you start to miss all that you had at home, like your friends at home, or your kitchen, or having a goddamn garbage disposal. It’s part of the usual adjustment process, but it can leave you with questions about whether or not you did the right thing by moving halfway around the world. Eventually this is followed by another up, then downs, until you reach a homeostasis of expatriation, or just another middle ground.
Even New Zealand seemed to have it out for some of us. One day it was a “mufti day” which meant that the boy could wear whatever he wanted instead of his uniform. Deciding that he loved his uniform, he decided to accessorize only with his Stitch hat with the big flappy ears. He left the house to walk to the bus stop. Eric was drinking a cup of coffee on the balcony overlooking the street. Suddenly, he noticed a commotion below him. The seagulls had left their usual post on top of the street lights to dive towards our son. The boy was being bombarded by a flock of seagulls who apparently thought that he, in his hat, was some kind of tasty large worm. The boy ran down the sidewalk, frantically waving his hands over his head to ward off the gulls, who squawked in frustration at being blocked from their breakfast. An older man walking along the beach stopped and stared at the scene, while we howled with laughter.
As if to troll us, our new place is decorated with all sorts of seagull paraphernalia that seems to have been put up with a permanent sticking charm. The boy doesn’t wear his hat indoors here, for fear of calling out the avian demons. They’d probably leave their paintings to attack in the middle of the night.



The girl has melted into school, and is having a ball. While she hasn’t made a lot of friends yet, she bounces out of bed every morning so excited about going to class. She loves her teacher, and one thing we’ve seen is that creativity is far more valued here than it is at home. Her homework, or “home learning” as it’s called here, is entirely open. Every two weeks she gets a sheet of paper with a variety of options for home learning – you can choose artistic options, math options, writing – so that every kid can find something to interest them at home, but without the rote tasks that homework seems to be back home.
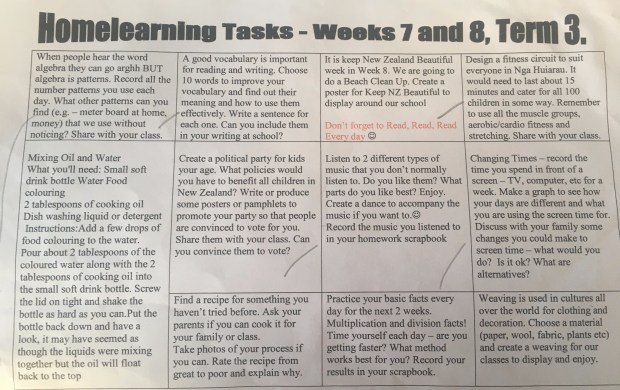
Homework for two weeks! You are expected to pick as many as you want to do and share at the end.
The boy is likewise enjoying school, and has a first playdate set up for this weekend. He was initially feeling a bit down about it, as NZ kids are quite sporty, and he’s…not. But he’s found his own little group of nerdlings as he does, playing chess in the school library at lunch and just this week has started introducing Dungeons and Dragons to his crew. His highlight of the last week was when he “accidentally” locked his shoes in the house when he left for the bus (we’d all already left for other destinations) and “had” to go to school barefoot. Upon arrival at school he was given the option of wearing a pair of the extra shoes they have at the office, but he declined.


As for me, the hospital work keeps on. Despite my years of experience back home, learning new medications and new systems leads me to feel like a new resident much of the time, which brings back all the traumatic PTSD I have related to that time and leaves me feeling unconfident.

These signs are all over the hospital. What sort of zombie apocalype are they expecting?!
So many times I’ll casually ask for something that Americans would see as completely normal, only to have it thrown back at me. I had a patient who had fallen and had a nasty scrape where he’d lost a fair amount of skin. Unthinkingly, I said, “let’s put some polysporin on it and cover it with a nonadhesive bandage.” The resident I was working with looked shocked. Absolutely SHOCKED. “We…shouldn’t do that. It’ll lead to antibiotic resistance.” I paused, knitting my brows, and replied, “so…you can’t just get an antibacterial ointment over the counter here? What do people put on cuts?” “We just tell them to put hydrogen peroxide on,” he replied. He then proceeded to look up antibiotic ointments that were available in the hospital, and after a search of five minutes finally came up with one that they had that used a different mechanism of action less likely to result in resistance. WHEW. I was kind of left feeling like, “Who’s the attending here?” and wanting to say indignantly “I AM! I’m the attending!”


Sometimes people think I’m a blinking idiot because it seems I can’t grasp a basic idea they’re talking about, when it’s just that I can’t understand their accent. They then go into details of whatever they were describing like I’m a moron, at which point I’m too embarrassed to correct them and say that it was their accent I couldn’t understand since of course, I’m the one with the accent. I had a patient who was telling me that he had “hot tack” a few years ago. Thinking that this was some Kiwi traditional therapy or something, I asked what “hot tack” was, only to get a quizzical look from my resident as she described “Hot tack? Well, it’s when the heart doesn’t get enough blood and then doesn’t work as well, and they get chest pain?” Oh. A heart attack. Great, now both patient and my resident think that I don’t know what a heart attack is. There goes any credibility I might have had.


That said, I continue to be amazed by the relative reasonableness of patients regarding their medical conditions. I’ve had far more conversations with ill people about their potential for death, and all of the elderly people I’ve talked with have expressed to me that they don’t want any aggressive measures to be taken and that they understand that this could lead to their death. These are different than conversations like this I have at home, where usually the question is asked to someone who is not in extremis, and even then limits to “what can be done” is not typically discussed. People will talk about not wanting to be resuscitated, or be put onto a breathing machine, but smaller discussions don’t often take place, and there is a different attitude towards end of life.
I do feel like I can be more relaxed overall with the patients here, chatting with them and able to bring more humor into our interactions. I’ll leave you with a story from last week.
I performed a procedure to remove excess fluid from someone’s belly, and it takes a while to get the fluid out slowly as we don’t have the handy vacuum sealed flasks here that whoosh it out in a matter of minutes. Over the 30 minutes I sat in the room, I chatted with the patient, a Maori person, and his daughter in the room. They live out in farming country, and I asked what type. “Cows, ship, pigs. All sohts of animuls.”
“Do you raise the sheep for meat or for their wool?”
“Wull. You can do it foh both…but listen to this. Theh was a farmah who hed his whole flock stolen! And thin two wiks latah, the entiah flock was returned to him, but they’d all bin sheahed! I said to myself, ‘theyah’s a man who knows the price of wul!’”
“Wait,” I said, “They brought the sheep back and no one noticed?”
“Oh yeah!” the daughter said, “And that’s when I said you know thet wasn’t no Mowri pehson stealin’ the ship because we would have kept those ship and fed them to our families!”
-s

Hope you’re all keeping a journal- too funny!
Atticus, I’m glad you’re favorite hat 🎩 survived!
Love you all😍
LikeLiked by 1 person
Poor Atticus! Finn and I had a good laugh over that story!
Arty
LikeLiked by 1 person
Eric had a better view than me and was dying of laughter!
LikeLike